Guest post by Dean Spears
A child’s height is one of the most important indicators of her well-being. Height reflects the accumulated total of early-life health, net nutrition, and disease. Because problems that prevent children from growing tall also prevent them from growing into healthy, productive, smart adults, height predicts adult economic outcomes and cognitive achievement.
Researchers studying height have long been puzzled by a paradox: Among developing countries, differences in average height are not very well explained by differences in income. In particular, children in India are shorter, on average, than children in Sub-Saharan Africa, even though Indians are richer on average.
What could explain this paradox? Because addressing widespread stunting is a health and economic policy priority, understanding determinants of children’s height is important. In a recently released Policy Research Working Paper (WSP 6351) I explore evidence for one possible explanation: open defecation. More than a billion people worldwide defecate openly without using a toilet or latrine. India, with some of the world’s worst stunting, also has one of the very highest rates of open defecation: more than half of the Indian population does not use any toilet or latrine.
Evidence in the medical and epidemiological literature has documented that germs in feces can stunt children’s growth. This is in part due to diarrhea, and in part due to enteropathy: chronic changes in the lining of the intestines that make it harder for the body to use nutrients. Well-identified econometric papers have also shown a causal link from sanitation to child height. For example, in a paper coauthored with Jeffrey Hammer about an experiment done in partnership with the World Bank Water and Sanitation Program and the government of Maharashtra, we find that a program that promoted rural sanitation also caused children to grow taller. Therefore, this new paper asks the quantitative, accounting question: how big is the effect of sanitation on child height? Big enough to account for important differences?
Open defecation around the world
Are the countries where many people defecate openly the same countries where the most children are stunted, and the average child is shortest? Yes, as demonstrated in the graph below. Cross-country differences in sanitation linearly explain 54 percent of the international variation in average child height.
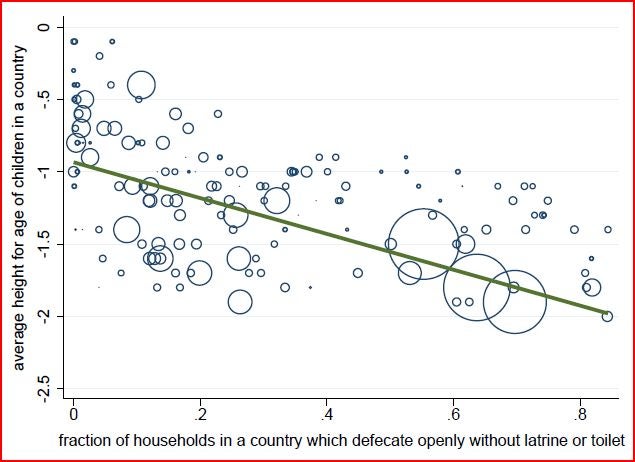
Each circle in this graph is a collapsed round of a Demographic and Health Survey, therefore, each represents one country in one year. The size of the circles is proportionate to the population of the country in that year. For example, the three largest circles at the bottom-right of the graph represent India in 1992, 1998, and 2005 – the three years when India had a DHS survey. One striking fact is that India’s circles fall on the trend line. Indian children are very short by international standards, but are exactly as short as widespread open defecation in India predicts.
Further analysis in the paper suggests that the association between child height and open defecation is not merely due to some other coincidental factor. It is not accounted for by GDP or differences in governance, female literacy, breastfeeding, or other forms of infrastructure such as availability of water or electrification. Because changes over time within countries have an effect on height similar to the effect of differences across countries, it is safe to conclude that the effect is not a coincidental reflection of fixed genetic differences.
Good toilets make good neighbors
If open defecation is indeed keeping children from growing to their genetic potentials – rather than merely being coincidentally correlated with height – we would expect open defecation to be more important for health outcomes where children are more likely to encounter whatever fecal germs are introduced into the environment. This means that population density should matter: living near neighbors who defecate openly is more threatening than living in the same country as people who openly defecate far away.
The graph below confirms that this is the case: child height is even more strongly associated with the average number of people per square kilometer in a country who practice open defecation. The density of open defecation per square kilometer, in this simple linear graph, can account for 64% of international variation in child height.
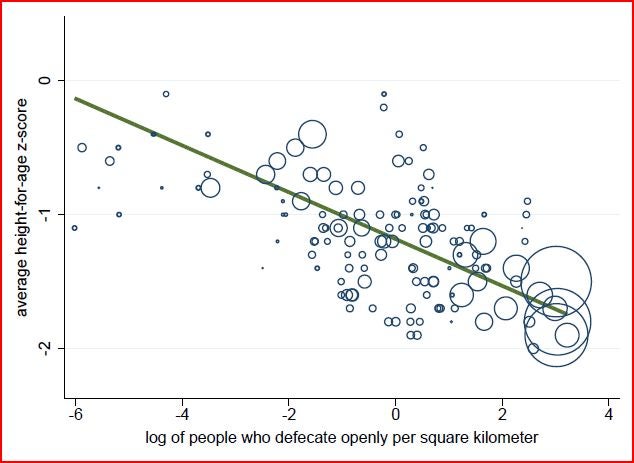
The graph plots the same 140 country years as before, and again the three large circles represent India. Once again, stunting among Indian children is no surprise: they face a double threat of widespread open defecation and high population density.
An “Asian enigma”?: Height differences between India and Africa
Households in India are less poor, on average, than households in Sub-Saharan Africa, but children there are shorter. Stunting is common even among relatively well-off families in India. However, widespread Indian stunting is not due to genetics: Indian babies who move to developed countries in early life grow much taller.
Because of the effect of open defecation on stunting, we can estimate how tall Indian children hypothetically would be if exposed to the better sanitation profile in Africa. Decomposition results in the paper – in the spirit of Blinder-Oaxaca – show that sanitation differences are able to completely explain this gap. Constructing a counterfactual sample of children’s heights in India’s most recent DHS weighted to match the exposure to open defecation in a set of pooled DHS surveys from Sub-Saharan Africa can eliminate the India-Africa gap.
This suggests that sanitation is very important, but it isn’t everything important. For example, in joint work with Diane Coffey and Reetika Khera, we show that children of women in India with lower social status grow less tall, identifying the consequences of intrahoushold rank by taking advantage of special properties of rural joint Indian families. Because these children are in the same household, the presumably are exposed to essentially the same sanitation environment. Further, because Indian households are richer, Indian children would be expected to be taller than African children, beyond merely eliminating the gap. Moreover, even matching African levels of open defecation, children in both regions would be much too short.
Stunting is often referred to as “malnutrition.” Sometimes in policy debates, this is taken to imply that the solution is to provide more food. But what these results suggest is that the disease environment is an important cause of “malnutrition,” too. If so, then far from merely a concern of infrastructure specialists, open defecation would a priority for health and nutrition policy – and for children’s well-being and the productivity of the next generation of workers.
Dean Spears is a PhD candidate in economics at Princeton University and a visiting researcher at the Delhi School of Economics. He is a co-founder of rice – online at www.riceinstitute.org – a research organization based in India and focused on the economics of early life health and human capital accumulation. He splits his time among Princeton, NJ; Delhi; and Sitapur, Uttar Pradesh.

Join the Conversation