
In Indonesia, chronic malnutrition is widespread with more than one-third of young children being stunted. Despite the reduction of the poverty rate from 16.6% to 11.4% from 2007 to 2013, the rate of stunting amongst children under the age of five has remained alarmingly high, exceeding 37% in 2013, although that figure has declined in the last two years. Stunting has important lifelong consequences for health, as well as for cognitive development, education, human capital accumulation, and ultimately for economic productivity.
However, to reduce stunting it’s not only important to focus on the health sector. It also requires improvements in other sectors such as agriculture, education, social protection, and water, sanitation, and hygiene (WASH). As originally emphasized by the UNICEF conceptual framework, to ensure that a child receives adequate nutrition depends on four critical factors: care, health, environment, and food security, areas that straddle multiple sectors.
Naturally, interventions to reduce childhood stunting that target one particular sector may not achieve the desired impacts if they aren’t complemented with appropriate measures across other sectors. For example, integrating nutritional considerations in the agricultural sector is unlikely to take into account the fact that WASH services may be poor and inadequate in some communities. As a consequence, the impacts of such interventions on key nutrition outcomes could be impeded considerably by the absence of adequate WASH facilities. The impacts of the same nutrition-sensitive agricultural interventions could be enhanced considerably if they were to be accompanied by simultaneous improvements in the water and sanitation facilities in the same communities.
Given such interlinkages, we launched a new report with the National Institute of Health Research and Development (NIHRD) of the Ministry of Health of the Republic of Indonesia that lays the groundwork for a more effective multi-sectoral action on reducing stunting in Indonesia. The report provides a lens for a more systematic monitoring of the progress in access to the four main drivers of child malnutrition. It also identifies potential “binding constraints” to reduce child stunting.
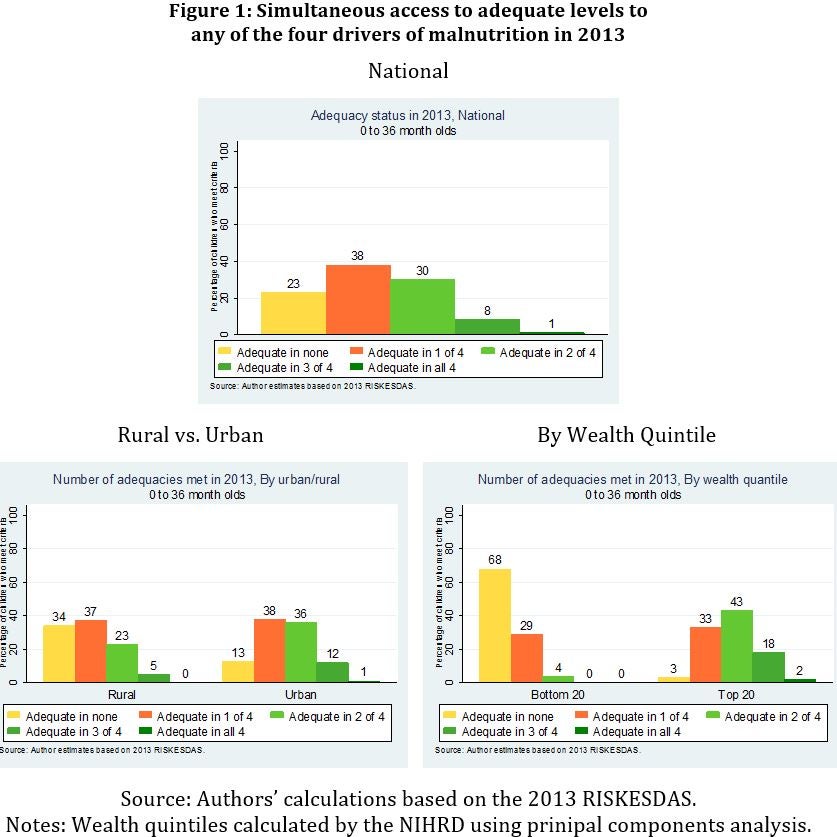
The analysis reveals that in 2013, 23% of the children between 0 and 3 years did not have adequate access to any of the four determinants of nutrition, down from 39% in 2007. On the other end, less than 1% of children had simultaneous access to all four of the underlying determinants of nutrition (see Figure 1). The differences in simultaneous access to two or more drivers become larger between rural and urban areas and by quantile of wealth.
The low proportions of children with simultaneous access to more than one of the drivers of nutrition suggests that the success of sector-specific nutritional initiatives could be constrained by inadequate access to the other underlying determinants of malnutrition.
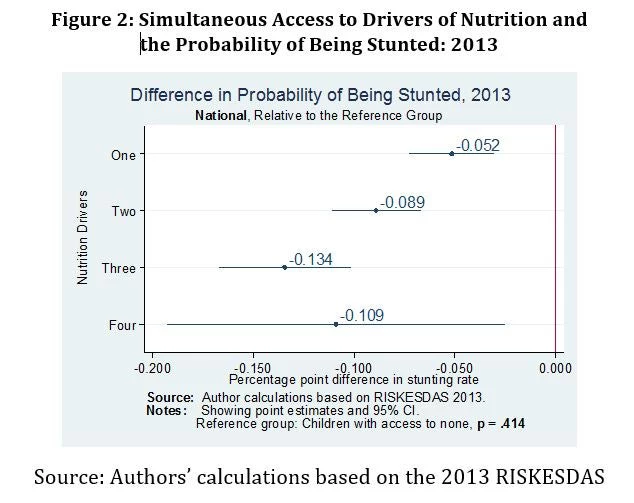
Further analysis also reveals that simultaneous access to two or more of the four key determinants of nutrition is associated with a decrease in the likelihood of a child being stunted (see Figure2). The likelihood that children between 0 and 36 months of age are stunted is lower when they have simultaneous access to adequate levels to two of the four drivers of nutrition and is even lower among children with simultaneous access to adequate levels to three of the four drivers of nutrition (Figure 2).
In combination, these results suggest that progress toward reducing stunting in Indonesia can be enhanced by coordinated multi-sectoral interventions that address effectively the four key underlying determinants of nutrition. For example, nutrition-sensitive intervention in the agricultural sector, such as giving incentives to poor and undernourished households to grow fruits and vegetables in their own home gardens, could be accompanied by coordinated interventions to improve the WASH services prevailing in these communities. Such coordinated efforts would not only decrease the incidence of diarrhea and illnesses associated with an inadequate environment but also strengthen the positive nutritional impacts of consuming micronutrient-rich fruits and vegetables.
The report also highlights the numerous data gaps that need to be addressed for a more informed and better coordinated approach across line ministries in Indonesia. In essence, it concludes that for Indonesia to fight against childhood malnutrition requires clarity and prior agreement on the common yardstick used among the different sectors involved so that the country can achieve efficient improvements in its policies.

Join the Conversation