Also available in: Español | العربية
Paul Farmer recently wrote in this space about Essential Surgery, the first volume released of nine expected in the Disease Control Priorities, 3rd edition series. He characterized that book as shining a spotlight on a long-neglected topic in global health and gave these reasons for the neglect: “Prevailing wisdom dictated that the surgical disease burden was too low, surgical expenses too high, and delivery of care too complicated.”
Substitute “cancer” for “surgery” and you have the topic and the challenge of the second published DCP3 volume. Cancer rivals surgery in its degree of global neglect and in Cancer, an equally compelling case is made for stepping up control efforts—including treatment and palliative care in addition to prevention—even in the poorest countries. And of course, surgery is a core component of cancer treatment—more cancer has been cured by surgery alone than by any other means.
Start with the cancer burden: As we reach closure on the 2015 Millennium Development Goals for child survival, and as life expectancy continues to rise in most countries, the population at risk for cancer grows. Of the 8 million cancer deaths each year worldwide, 5 million of them already occur in low- and middle-income countries (the large majority in middle-income countries). That proportion is increasing as is the proportion of all deaths that are caused by cancer. Not often appreciated is that age-standardized cancer death rates are declining in most countries, but the other major causes of death, both infectious and noncommunicable, are declining faster.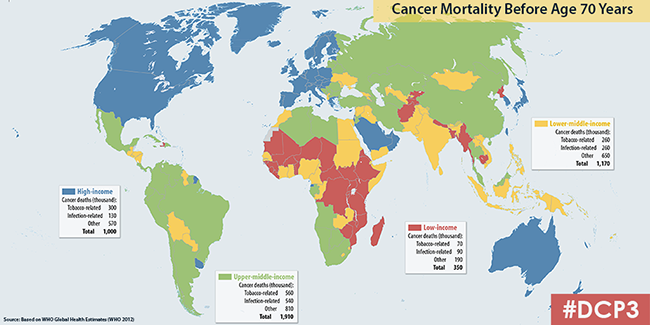
The fastest growing portion of the burden in low- and middle-income countries (LMICs) are the types of cancer caused by tobacco—arguably the most preventable common cancers. Just behind in preventability are two vaccine-preventable cancers: liver cancer caused by hepatitis B virus and cervical cancer caused by the human papillomavirus. Beyond that, however, the cancers that are becoming more common are, by and large, not preventable with today’s knowledge and interventions: breast cancer, colon cancer, pancreatic cancer, most leukemias and lymphomas and many less common cancers. However, many of these are highly curable, especially when diagnosed early (stages 1 and 2). Without treatment, most are invariably fatal.
The full array of interventions—surgery, radiotherapy, chemotherapy, endocrine therapy—is needed for many common cancers (breast cancer is a good example). While many early-stage cancers can be can be cured by surgery alone, for others, cure is possible only when some other modalities are added. When that is the case, starting treatment with less than a full complement can mean inflicting harm without much benefit.
A major hurdle in cancer control is the large proportion of cancers diagnosed at late stages in LMICs, when cure is impossible even with state-of-the-art treatment. How can the curve be shifted? We see this as a feedback loop: as people begin to be cured, societal attitudes toward cancer begin to change and people are more willing to come forward for evaluation when they detect something amiss, even without formal large-scale screening programs. It may be a slow process, but building up infrastructure and especially the human resource base for cancer control is also slow. The sooner the process starts, however, the sooner it will gain population-wide strength.
Among the most curable of cancers, even if not the most numerous, are some of the common childhood cancers, particularly the leukemias and lymphomas, retinoblastoma, Wilms tumor and some others. Curing children—cost-effectively and affordably—is clearly a good thing and also sends a powerful message for that feedback loop needed to change public attitudes about cancer.
Even in the longer term, once treatment is widely available, cancer will be a common cause of death in rich and poor countries—common and often painful. The DCP3 volume makes the case—yet again—for a rapid expansion of pain control, including opioid drugs, even in the poorest countries. A model program in Uganda that began more than two decades ago, and a small handful of others, demonstrate unequivocally that it is possible to provide pain control for dying cancer patients at home, even in rural Africa and Asia.
The foreword to DCP3 Cancer was written by Professor Amartya Sen, himself a cancer survivor as a young man, who considers himself among the few lucky ones of his time and place. He ends with this:
The lesson that emerges from the well-aimed empirical analyses presented in this volume is not only that a major difference can be made in the incidence, management, and elimination of cancer, even in the poorer countries of the world, but that this can be done in cost-effective and affordable ways. Understanding and determination are the deficiencies most in need of change.
This is, ultimately, a cheerful book on a very grim subject. It is also a hugely important invitation to action.
Follow the World Bank health team on Twitter: @WBG_Health

Join the Conversation