This is the thirteenth in this year's job market series.
Malthus’ pessimistic view of development was that improved living standards would be cancelled out by population growth in the long run. However, this scenario stands in contrast with historical and current experience, as developing countries have successfully escaped from this trap, with a slow-down in population growth. The modern experience of developing countries is thought to be best explained by increases in life expectancy, which cause people to have fewer children. However, causal estimates in support of this hypothesis remain rare (Galor 2012).
My job market paper (which is joint work with Sonia Bhalotra and Atheen Venkataramani) sheds light on this question. We examine the introduction of the first antibiotics in the United States in the 1930s, which caused sharp reductions in child mortality from pneumonia.
We find that women reduced their fertility when child survival improved, consistent with popular growth theory. Interestingly, we also find an increase in the number of women who remained childless. This is a puzzling finding: modern economic theory posits that improvements in child health will make it more - not less - attractive to have at least one child (Becker and Lewis 1973, Aaronson et al. 2014).
This puzzle can be resolved by thinking about the other choices women have to make. The story is simple: when child survival improves, there is less of a need to start having children early in life, since each pregnancy is more likely to succeed. This is reinforced by women wanting fewer children. Thus, women delay fertility and enter the labor market. Once childbearing has been put on hold, however, a range of shocks can cause a woman to end up childless. Consistent with this hypothesis, we find that women had children later, were more likely to be in the labor market, and achieved better occupations, after the decline in child mortality.
Developing countries today are likely to be subject to similar forces, as child mortality continues to fall from previously high levels (Liu et al. 2016). We can therefore learn from our results about the potential impact of health policies on fertility, and also about how such policies can help women achieve economic independence.
The setting and research strategy
Sulfonamide (sulfa) drugs were introduced in 1937 and changed the standard of modern medicine. They treated major bacterial diseases including pneumonia, the leading cause of child mortality, and a “sulfa craze” followed, with 10% of the US population treated annually by 1941. Mortality rates from pneumonia – which was predominantly a disease of childhood – declined in the United States by 17-32% with the advent of sulfa drugs (Jayachandran, Lleras-Muney and Smith 2010).
We exploit cross-state variation in mortality rates before the introduction of sulfa drugs. States initially most burdened by pneumonia mortality experienced the largest declines in mortality rates after the introduction of sulfa drugs, yielding a “continuous difference-in-difference approach” similar to Acemoglu and Johnson (2007) and Bleakley (2007).
Effectively, we investigate whether the convergence in levels of pneumonia mortality across US states after 1937 is mirrored in the fertility and labor market behavior of women. We fail to reject the null hypothesis of parallel trends and run a number of checks that address competing hypotheses for the patterns we observe, including the role of WW2, the Great Depression, and mean reversion.
Findings
We find that the decline in child mortality due to antibiotics led to a decline in fertility, with a decrease in the number of women with three or more children and, strikingly, an increase in the number of childless women. For the average woman in our sample, the probability of childlessness at age 40 increased by 4.6% relative to baseline.
Next, we estimate a survival model of motherhood and find that the time to motherhood increased with child mortality decline: for every additional year of exposure to sulfa drugs, the average woman was 5.9% of baseline less likely to transition out of childlessness. Women delayed fertility in response to child mortality decline.
Turning to labor market responses, we show that when child survival improved, women were 7% more likely to be in the labor force, their occupational scores increased by 6.6% and their working hours increased by 9% of baseline. Interestingly, there was a smaller reduction in marriage probability of 1.7%, suggesting that the marriage market was not the key mechanism that linked child mortality and childlessness.
Labor force participation among married women increased from 10% to 25% in the 1930s: women who wanted to have careers were now able to do so. Previous work has attributed this to the rise in high school completion (Goldin 2006), but our results suggest that child mortality decline may have contributed a substantial share of this rise.
Understanding the link between childlessness and labor force participation
Fertility and labor market choices are clearly made together: having children can have implications for returns to human capital, and the need to organize childcare can increase the cost of having children for working women.
We argue that the puzzling effect of child mortality decline on childlessness is easy to understand when taken together with the effects on fertility delay and labor market participation. The mechanism is intuitive: as child mortality declines, women need to spend less time childbearing. This gives them the option to do other things, such as work. Thus, women may opt to delay childbearing and remain in or enter the labor force.
Being in the labor force opens the door to experience and circumstances: for example, women may learn that they really like to work. Or, they may do very well at it, increasing their opportunity cost of exiting the labor force. Alternatively, biological factors may kick in if fertility is delayed too long. These circumstances can eventually result in childlessness, even if this was not the woman’s initial intention.
This study is the first to link child mortality with delay and childlessness; however, surveys exist that document childlessness as a result of women having careers in the 1970s (Goldin 2004), 1990s (Goldin 2006) and even in the US in 1936 (Popenoe 1936). My job market paper proposes a theoretical model that explains when child mortality decline leads to delay, labor market participation and eventual childlessness.
Implications for policy?
The context of this study – the US in the 1930s – matches the burden of child illness and fertility behavior in modern developing countries. Fertility remains high at 4.7 births per woman on average in Africa, for example (United Nations 2015). Worldwide, pneumonia continues to be the leading cause of death among children: 6 million under-5 children continue to die every year (Liu et al. 2016). In Africa in 2015, pneumonia caused more deaths among children under 5 than malaria, and lower respiratory tract infections were the most common all-age infectious cause of death, eclipsing deaths from malaria and HIV/AIDS (WHO 2015). While eighty years have elapsed since the invention of antibiotics, the average consumption of antibiotics in West Africa is approximately 90% lower than in the United States, suggesting poor access (Hogberg et al. 2014).
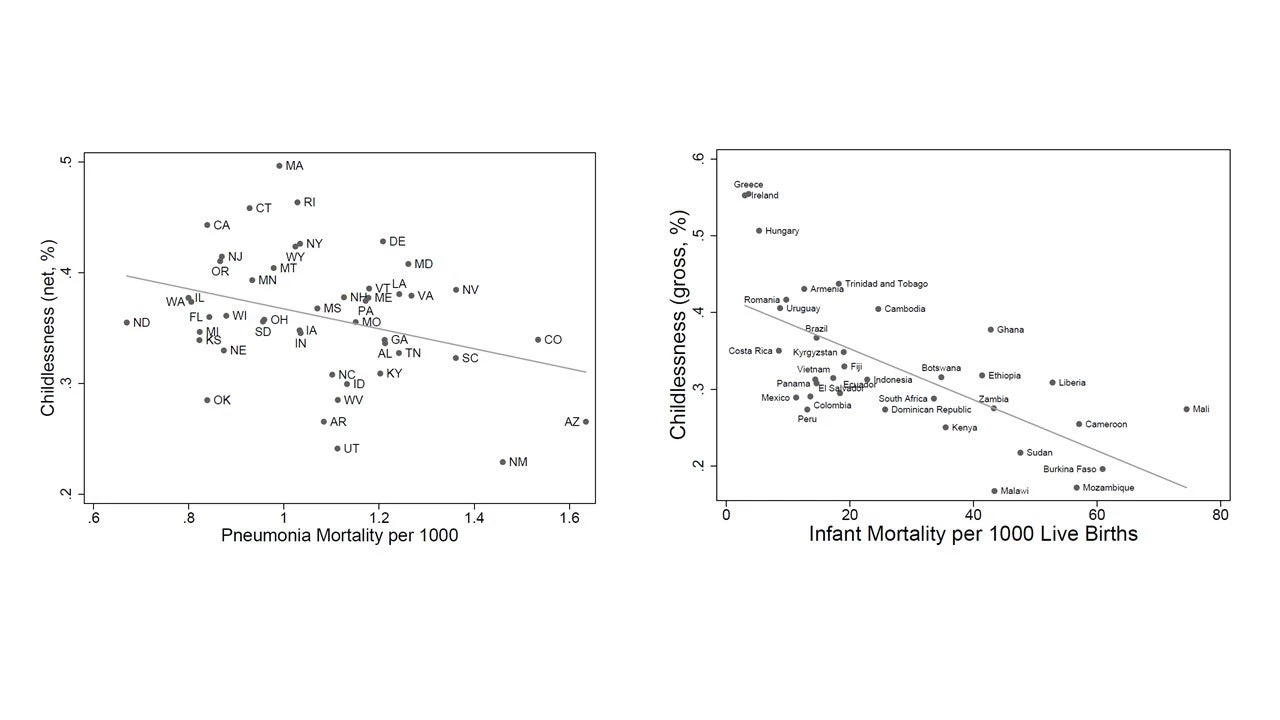
To highlight the broader relevance of our findings, we estimated the correlation between child mortality and childlessness across U.S. states in 1930 (left, pneumonia), and across countries in 2015 (right, all-cause). In both figures, we see a negative correlation between child mortality and childlessness.
Our results suggest possible knock-on effects of child mortality decline on childlessness, women’s work and marriage. Specifically, we provide further proof that child mortality decline (combined with viable job opportunities) may have the potential to "liberate" women in developing countries into work and away from long periods of time spent childbearing.
Selma Walther is a postdoctoral fellow at the University of Warwick and holds a PhD from the University of Cambridge. You can read about her research here.

Join the Conversation