Today the Maternal Mortality Estimation Inter-Agency Group (MMEIG) released a report on the global and country maternal mortality estimates for 2013. Globally, maternal mortality ratio (MMR) decreased from 380 maternal deaths per 100 000 live births in 1990 to 210 in 2013. Although this 45% decline is far less than the expected 75% decrease between 1990 and 2015 in order to achieve the fifth millennium development goal (MDG 5), 19 countries were reported to have already achieved MDG 5: Belarus (96%), Maldives (93%), Bhutan (87%), Cambodia (86%), Israel (84%), Equatorial Guinea (81%), Poland (81%), Lao People's Democratic Republic (80%), Romania (80%), Bulgaria (78%), Estonia (78%), Timor-Leste (78%), Eritrea (77%), Cabo Verde (77%), Latvia (77%), Oman (77%), Lebanon (76%), Nepal (76%) and Rwanda (76%).

The report also noted that of the 183 countries and territories included in the estimation exercise, only 67 countries mostly from high income countries had MMR directly computed from civil registration data (Figure 1). The remaining countries had MMR estimated from a multilevel regression model. The range of uncertainty or confidence intervals of the MMR estimates from statistical models are so wide that they cannot be used for short term monitoring and evaluation of maternal health programs (Table 1). Neither do they produce MMR estimates at sub-national level to inform planning and implementation of programs. Considering that the MMR estimates from household surveys such as the demographic and health surveys (DHS) have limitations (such as capturing pregnancy-related deaths instead of maternal deaths, and providing estimates for several years prior to the survey instead of the reference year [Table 1]), the MMEIG includes the DHS data in a statistical model in order to obtain more robust MMR estimates. This sometimes puts countries in a quandary as to which one to use in official reports.
Figure 1. Map with countries showing the source of data for maternal mortality estimates, 2013
Table 1. Comparison of 2013 MMEIG and 2012 DHS MMR estimatesa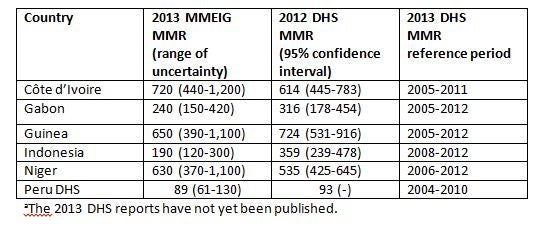

Measuring MMR (number of maternal deaths during a given time period per 100 000 live births during the same time period) requires universal birth and death registration as well as attribution of cause of death. For instance, birth registration coverage can be readily increased to be at par with other services with high coverage rates such as immunization and use of antenatal care. As shown in Figure 2, birth registration coverage tends to lag behind coverage of antenatal care and DPT1 immunization. Thus, existing maternal and child health services can be used as entry points to boost birth registration such as creating awareness among pregnant women during antenatal care, immediate birth registration of all institutional births, and ensuring all children who are vaccinated at 6 weeks for DTP1 vaccination are registered. Additionally, birth registration can be included in the list of incentivized indicators in results-based financing programs. Further, establishing maternal death surveillance and response systems will provide the require data on maternal deaths.
The World Bank together with other development partners (ADB, AfDB, African Union, BMGF, DFATD Canada, CDC, CEPA, CGDEV, IADB, PARIS21, Plan International, Statistic Norway, UN Every Woman Every Child, UN Statistics Division, UNECA, UNESCAP, UNESCWA, UNFPA, UNHCR, UNICEF, USAID, and WHO) and country representatives (Bangladesh, Burkina-Faso, Ethiopia, Mozambique, and Philippines) is developing a Global Civil Registration and Vital Statistics: Scaling-Up Investment Plan 2015-2025 to help galvanize action and mobilize additional resources for strengthening CRVS in low and middle income countries. The plan will released prior to the Toronto Summit Saving Every Woman and Every Child in May 28-20, 2014.
Figure 2. Birth registration lags behind antenatal care and DPT1 immunization, DHS surveys

Follow the World Bank Health team on Twitter: @worldbankhealth

Join the Conversation