
The Domestic Resource Mobilization (DRM) collaborative cohosted its recent meeting with the Efficiency Collaborative on February 27-28 in New Delhi, India. This was the third in-person meeting of the DRM collaborative .
Overview
India was the host and catalyst for the first-ever meeting of the JLN- Returning to India allowed participants to leverage learnings from recent reforms, including the National Health Mission (NHM) and the Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB PM-JAY), one of the world’s largest government-sponsored schemes designed to provide financial protection to 100 million poor and vulnerable families. The discussion featured Ms. Preeti Sudan, Secretary, Ministry of Health and Family Welfare, Government of India, and Dr. Indu Bhushan, CEO National Health Authority, Pradhan Mantri Jan Arogya Yojana. AB PM-JAY covers inpatient secondary and tertiary care at empaneled public and private facilities and is financed by a new ‘cess’ -- i.e., an additional soft earmarked income tax – of about 1% that largely falls on wealthy non-beneficiaries. Earlier in the day, a thought provoking introduction to India’s health sector came from the JLN country core group chair, Mr. Alok Saxena, Joint Secretary of the National AIDS Control Organization, Ministry of Health and Family Welfare, who shared the dais with Jorge Coarasa, Acting Country Director of the World Bank India office.The group then reviewed the concept of DRM and its different components, including a presentation on DRUM, Domestic Resource (DR) Use (U) and Mobilization (M), for UHC. DRUM emphasizes the efficient use of resources for health and was a good segaway to the discussions of the two collaboratives.
The meeting also examined inventories of DRM-related resources including the JLN WHO-R4D database on earmarking for health, and progress on a “learning laboratory” in Sudan- country-led meetings with various Ministry of Health, Ministry of Finance, and other stakeholders, to discuss communication challenges and share targets for investing in health.
The following day examined DRM misconceptions, including whether public health spending increases automatically when reprioritization occurs. Participants also discussed determinants of reprioritization, featuring a draft questionnaire that assesses country factors contributing to reprioritization and its role for DRM. An update was provided on progress with a messaging guide to inform dialogue around DRM, as well as narrative summaries describing countries health and public financing context.
Key take-aways
Understanding DRM is a critical part of fiscal space for health. Fiscal space for health can be gained through conducive macroeconomic conditions that lead to increases in the size of the economy or the government in relation to gross domestic product; reprioritization of health through a greater share of government budget; health specific revenues; development assistance for health; and efficiency gains. DRM is a subcomponent of fiscal space that focuses on the first three elements.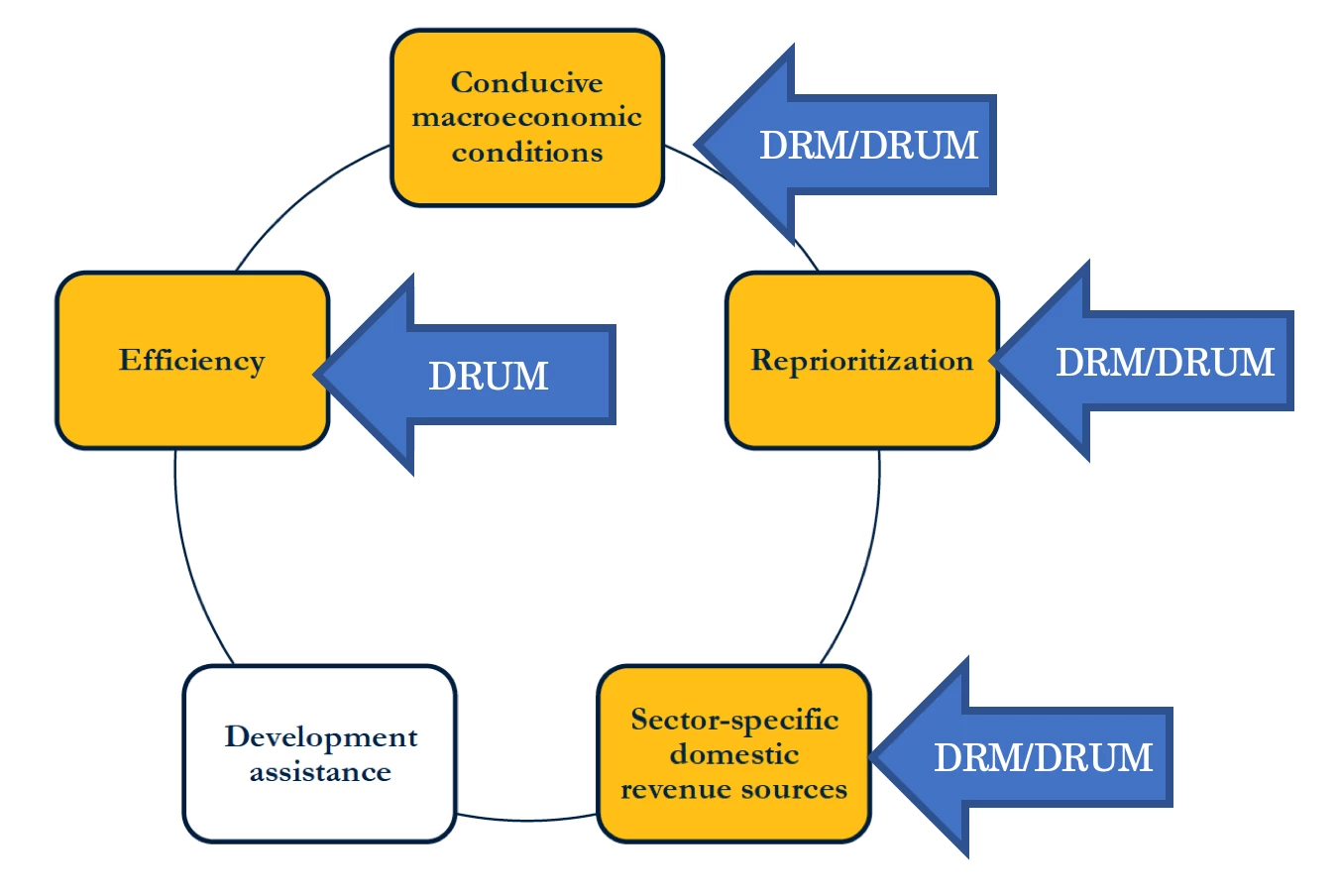
It is important to both mobilize domestic resources, and improve the efficiency and equity in the use of resources. The DRUM framework links DRM and efficiency and can be a useful way to think about fiscal space as it helps make efficient and equitable use of resources more explicit, and as a complement to DRM. This framework was developed to learn from the past and foster innovations to ensure accelerated process towards Universal Health Coverage.
Inventories of DRM for health efforts remain underleveraged. The few efforts that qualify as inventories - from learnings and tools from the USAID HFG project, to data on tobacco use and prevention policies and tobacco tax simulation models to the JLN WHO-R4D earmarking database - were unknown to most participants. More work is needed to assess whether and how countries use this information, how to improve accessiblity, and identify other inventories.
Although evidence remains limited, prioritization of health in the budget seem to be positively correlated with democratization, CSO involvement and female political participation; while weak governance is negatively correlated. The impact of development assistance for health (DAH) on domestic resource mobilization remains debatable.
Dialogue between ministries of finance, ministries of health and other stakeholders is critical to breaking down the communication divide. Helping finance and health practitioners to find common language can impact DRM for health. Through the learning lab, stakeholders gained a better understanding of mutual constraints and opportunities, and were able to establish a platform for discourse across finance and health, and at Federal and State levels.
Next steps
DRM for health continues to be a high priority topic. To respond to demand, the collaborative will complete these deliverables: a messaging guide, narrative summaries, case studies on prioritization, and a learning lab toolkit. The team will also continue to explore how to strengthen and highlight existing inventories of DRM efforts.
This post is a joint product of the authors and a broader facilitation team including Aditi Nigam, Emiko Masaki, Lydia Ndebele, Somil Nagpal, and Valerie Glibert T. Ulep.



Join the Conversation