 Menstrual Hygiene Education
Menstrual Hygiene Education
With the Sustainable Development Goals (SDGs) came an expansion in the ladder used to measure WASH targets, and an added focus on capturing inequalities in access to services.[1]”
A central way in which gender inequalities unfold in the WASH sphere is through the prevalence of a sanitation infrastructure which does not allow women to exercise proper menstrual –hygiene management (MHM). According to the WHO/UNICEF Joint Monitoring Programme (JMP), for women and girls to have access to adequate MHM, to be able to manage their menstruation hygienically, they must have access to:
“…clean menstrual management material to absorb or collect menstrual blood, that can be changed in privacy as often as necessary for the duration of a menstrual period, using soap and water for washing the body as required, and having access to safe and convenient facilities to dispose of used menstrual management materials. [2]”
Inadequate access to MHM has a wide range of social repercussions. Although the nature of the causal connection is unclear, a women’s poor access to MHM is associated with a number of, primarily non-sexually transmitted, reproductive tract infections (RTIs).[3][4][5] Moreover, the social taboo[6] associated with menstrual hygiene, coupled with how access to sanitation facilities deficient in MHM can increase the amount of time women spend catering to their menstrual hygiene needs, may prevent social inclusion, and stop women from advancing their human capital accumulation.
To shed light on the matter, the JMP has been pushing to standardize, and expand, a module with additional information on MHM, to be administered across nationally representative household surveys.[7] The questions have already been tested in a number of countries, and recently released estimates from UNICEF’s Multiple Indicator Cluster Surveys (MICS) – years 2017 and 2018 – include revealing information on the status of menstrual hygiene.
Consider: Although there is significant variation across countries, the data suggests overall high levels of access in several aspects of MHM. More than eighty percent of women in four out of the six countries reviewed have access to menstrual hygiene materials, and a private place to wash and change. The only exception to this is the country of Tunisia, and the rural areas of Laos (Figure 1).
Figure 1)

The high estimates from Figure 1 should be taken with a grain of salt, as they do not ask about access to water and soap in the space used for menstruation, nor do they take into account the safety, cleanliness, and hygiene of the sanitation facilities used for MHM. For instance, data from the nationally-representative PMA2020 health and family planning surveys, funded by the Bill and Melinda Gates Foundation, and collected in more than eleven countries in Asia and Africa, found that: across countries, the sanitation facilities used by women for menstrual hygiene “are not safe, clean or private and frequently lack water or soap and that relatively few facilities meet all these criteria.[8]”
A large percentage of women reported that their last menstruation interfered with their day-to-day activities. For instance, around twenty percent of women in Sierra Leone, and seventeen-eighteen percent of women in Suriname reported that their last menstruation prevented them from attending social activities, school or work. (Figure 2)
Figure 2)
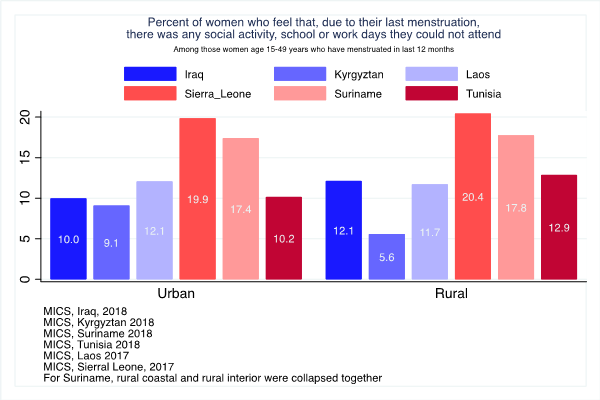
The high percentages presented in Figure 2 are eye-opening, and raise the need for additional research, both quantitative and qualitative, to be conducted to unfold some of the patterns driving the connection between MHM and social exclusion.
JMP’s push for addition of a menstrual hygiene module as part of MICS data is a valuable first step in helping shed light on a topic of central importance to women’s health, to social inclusion, and to human capital accumulation.
In addition to pushing for the further expansion of the menstrual hygiene module, a whole breadth of additional information,[9] is required to get a more complete, and nuanced, picture on the status of MHM in developing countries.
Notes:
[1] SDG goal 6.2 reads: “By 2030, achieve access to adequate and equitable sanitation and hygiene for all and end open defecation, paying special attention to the needs of women and girls and those in vulnerable situations.
Progress on household drinking water, sanitation and hygiene 2000-2017. Special focus on inequalities. New York: United Nations Children’s Fund (UNICEF) and World Health Organization, 2019.
[3] Sumpter, Colin, and Belen Torondel. “A Systematic Review of the Health and Social Effects of Menstrual Hygiene Management.” PLOS ONE, Public Library of Science, 16 Apr. 2013, journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0062004
[4] Das, Maitreyi Bordia. 2017. “The Rising Tide: A New Look at Water and Gender.” World Bank, Washington, DC.
[5] The meta-analysis by Colin and Torendel (2013) found that the MHM literature following an experimental or quasi-experimental design is limited, so the causal relationship between poor MHM and women’s health is not entirely understood. Additional empirical work, in the form of studies following an experimental design, is required to fully understand the causal mechanisms connecting MHM to RTIs.
[6] “Menstrual Hygiene Management Enables Women and Girls to Reach Their Full Potential.” World Bank, 25 May 2015, www.worldbank.org/en/news/feature/2018/05/25/menstrual-hygiene-management.
[7] The MHM module includes questions on the start of the last menstrual period, on materials and reusability of materials used, on ability of women to wash and change at home, and on whether menstruation interfered with women’s capacity to work or engage in social activities.
The module does not include questions on water and soap within the MHM facilities (although the surveys do include question on access to a sanitation facility with a handwashing station with water and soap), or on the reasons why menstruation might have interfered with a women’s capacity to work or engage in social activities.
[8] PMA 2020: Performance Monitoring and Accountability 2020. Measuring Performance, Informing Policy, Empowering Communities. John Hopkins Bloomberg School of Public Health, Bill & Melinda Gates Institute for Population and Reproductive Health. October 25, 2018
[9] Additional information on the presence of water and soap in menstrual-hygiene facilities, on the quality and cleanliness of the sanitation facility used for menstrual hygiene, on the relation between menstruation and social activities missed, to name a few,

Join the Conversation